
This is the third and final part of our Attention-Deficit/Hyperactivity Disorder (ADHD) series of posts. The first and second posts reviewed evidence-based treatments for children and adolescents, as well as for adults with ADHD. In this final post, we will be sharing why ADHD diagnosis isn’t as simple as you might think.
ADHD has seen significant media coverage this year with no less than 5 articles on The Straits Times and CNA covering it. Topics in vogue included awareness of ADHD in adults, supporting individuals with ADHD, how ADHD presents differently in girls and women, as well as what to do if you suspect ADHD.
Reading these articles in the news, one could easily be forgiven for assuming that ADHD is pretty underdiagnosed and missed by parents, teachers, and professionals alike. However, that impression is far from accurate. In fact, a recent 2021 systematic review has found quite the opposite. In their study (Kazda et al., 2021), the authors evaluated 334 published research articles and found evidence that ADHD was overdiagnosed and overtreated in children and adolescents. Epidemiological studies (studies which look at the percentage of a condition in the population) have also found that the percentage of the population who was diagnosed with ADHD was steadily increasing, almost doubling from 6.1% to 10.2% in just 8 years (Cabral, Liu, & Soares, 2020).
On one hand, we have narrative accounts in the news media suggesting an underdiagnosis and underidentification of ADHD in the population, while on the other hand, epidemiological studies and systematic reviews suggested an overdiagnosis and overidentification of ADHD. So what exactly is going on? A more accurate picture may lie in between: while there were individuals who fell through the cracks and were undetected, the overall trend suggested overidentification and possibly overmedicating. The could happen due to the fact that diagnosing ADHD is a highly varied process which often relied on the confidence and comfort of the diagnosing clinician. That is to say, overly liberal clinicians may diagnose ADHD more readily than more prudent clinicians, based on fewer sources of evidence. Overly cautious clinicians on the other hand may have a benchmark so high that few could get diagnosed.
The challenges surrounding more accurate and objective ADHD diagnosis has been discussed in professional and academic circles since the 1990s. This led to a paper published in 2005 by Gualtieri and Johnson questioning what exactly is the ‘Gold Standard’ for ADHD diagnosis. The fact that ADHD diagnosis had been pretty loose and varied explained why some individuals who were diagnosed with ADHD in childhood no longer met diagnostic criteria in adulthood (e.g. ‘low persistence’). It wasn’t because these individuals ‘outgrew’ their ADHD. Rather, the use of poorly validated diagnostic processes led to this observation. Sibley, Mitchell, and Becker (2016) explained that, “when applying empirically supported methods of diagnosis, the disorder persists into young adulthood for many people. … By eliminating reliance on [less empirically supported] methods, more individuals with childhood ADHD who show clear evidence of the disorder will be eligible to receive a diagnosis in adulthood, which might facilitate treatment of their symptoms and related impairments.“
The lack of consistent and robust diagnostic processes for ADHD has implications not only for those who are/may potentially be on on the ADHD spectrum, but also for those who try to game the system. It has been well documented that college students ‘fake’ ADHD symptoms to obtain prescription stimulants to improve their cognitive performance in school. In a study by Lucke and colleagues (2018), up to 6.5% of Australian university students misused stimulants for the purposes of improving their academic performance. Locally, The Straits Times had reported in 2013 of university students who pretended to have symptoms of ADHD to obtain Ritalin, a psychostimulant, to boost their cognitive performance in school.
Insofar we’ve discussed how the lack of standardized ADHD diagnostic protocols may have contributed to:
- An underidentification of ADHD in select individuals,
- A trend tending towards overdiagnosis and overmedicating across populations,
- Low persistence in diagnosis across time (diagnosed as a child but no longer eligible for diagnosis and treatment as an adult), and
- A potential for systematic drug abuse, especially amongst college students.
So how is ADHD diagnosed?
Diagnosis of ADHD
ADHD is a symptom-based diagnosis given to individuals who meet the following criteria:
- 6 or more symptoms of inattention and/or 6 or more symptoms of hyperactivity and impulsiveness (5 symptoms if aged 17 and above); and
- Symptoms must be present for a duration of at least 6 months, and developmentally inappropriate; and
- Symptoms must be present before the age of 12 years old; and
- Symptoms must be generalized across 2 or more settings (e.g. home, school, work, social activities); and
- Symptoms interfere with functioning or quality of life; and
- Symptoms cannot be explained by another mental disorder (e.g. mood disorder, anxiety disorder, dissociative disorder, or personality disorder).
While the diagnostic criteria is specific and explicit, the evidence required to substantiate meeting the criteria is non-specified. In fact, different clinical and professional practice guidelines recommend different tests and tools to substantiate a diagnosis of ADHD. This was clearly demonstrated in Gualtieri and Johnson’s article:

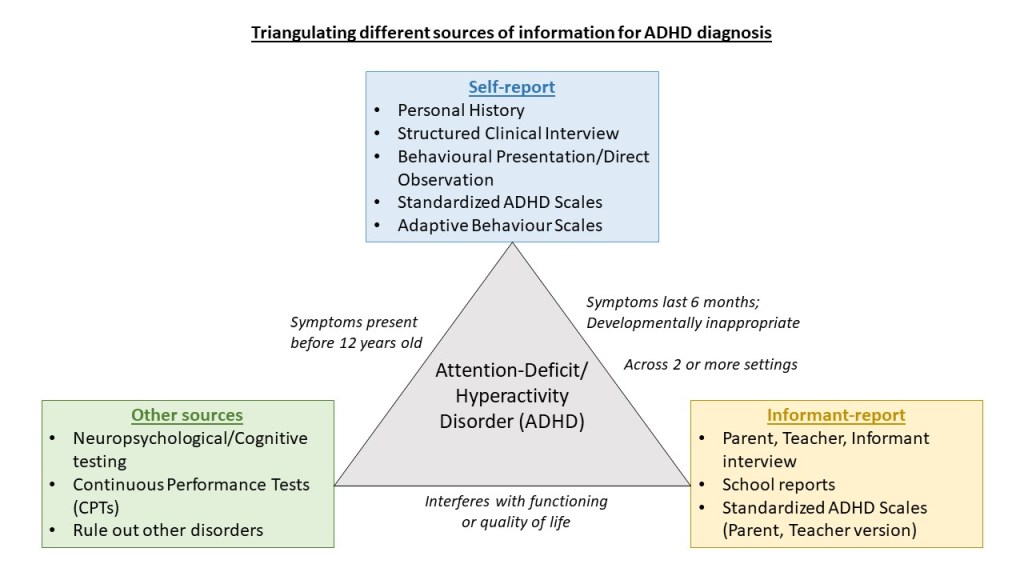
As seen above, different medical boards/associations recommend different sets of testing to be done in the diagnosis of ADHD. Nonetheless, a general rule of thumb in the diagnosis of ADHD would be to obtain subjective and objective information from multiple sources, and arriving at a diagnosis after triangulating the information (Martel et al., 2015). These sources of information may include:
- Personal history taking
- Structured clinical interview
- Behavioural presentation during assessment
- Parent, teacher, informant interview (or school reports)
- Administration of standardized ADHD scales (self-, and informant-reported)
- Administration of neuropsychological testing
- Administration of Continuous Performance Tests (CPTs)
While the use of structured clinical interview, neuropsychological testing, and CPTs in the diagnosis of ADHD was not recommended in some practice guidelines (Wolraich et al., 2019), studies have shown them to be useful. For example, both the DIVA 2.0 (Pettersson et al. 2015) and the SCID-5 ADHD module (Somma et al., 2019) have been shown to be clinically valid in ADHD diagnosis. A secondary benefit of using structured clinical interview compared to informal clinical interview is that it allows for alignment between clinicians, bringing us closer to a potential “gold standard” diagnostic process. While neuropsychological/cognitive testing and the CPT may not be useful as standalone diagnostic tools (Guo et al., 2020), research have shown that they are useful adjunct assessments (Nikolas et al., 2019). For example, Pettersson and colleagues (2015) found that neuropsychological testing “can provide important information in assessing the core variables in ADHD, especially of attention, activity, and impulsivity.” The use of CPT also contributed to diagnostic accuracy by increasing the specificity by 10% (e.g. increase the ability to identify true negatives).
Summary
In all, the diagnosis of ADHD is not an easy one. At present, no ‘gold standards’ exist to help clinicians better discern ADHD from neurotypicality. At best, we could only rely on multiple sources of information to refine our diagnostic acuity. Nonetheless, substantial variation exists regarding what constitutes ‘multiple sources of information’. If we are too lax and liberal, we run the risk of overdiagnosing and overmedicating. Bad actors with the intention of obtaining psychostimulants for academic benefits may also slip through the loosely guarded gates. Too strict, and we exclude a significant portion of legitimate cases who may not have the resources or capacity to fulfil all the requirements of a comprehensive ADHD diagnostic battery.
While history taking and the used of standardized ADHD scales are the norm, research findings have supported the use of structured clinical interview as well as neuropsychological testing/CPT in conjunction to subjective reports/informal interview and behavioral scales. Perhaps the elusive common standard we should all follow was already argued for by Gualtieri and Johnson in 2005 (p.51), “The ‘gold standard’ for ADHD diagnosis includes a comprehensive clinical history and examination, rating scales, direct behavioral observations, neuropsychological testing, and objective, comparative analysis of different drug effects.”
Eugene

2 thoughts on “Opinion/Commentary: Diagnosing Attention-Deficit/Hyperactivity Disorder (ADHD)”