
This is the second part of our ADHD literature review series. Today’s article focuses on evidence-based treatments for adults with attention-deficit/hyperactivity disorder (ADHD). For those looking for evidence-based treatments for children and adolescents with ADHD, you may find our previous article useful.
Today’s Wassup’ post will review 2 fairly recent meta-analytic and systematic review studies, one focusing on pharmacological treatment, while the other on non-pharmacological treatment.
Pharmacological Treatment for adults with ADHD
In the above study, researchers conducted a meta-analysis involving 64 randomised controlled trials (RCTs) examining the efficacy of pharmacological treatments (amphetamine salts, atomoxetine, bupropion, clonidine, dexmethylphenidate, guanfacine, lisdexamfetamine, methylphenidate, modafinil) against a placebo across more than ten thousand adult participants.

Findings:
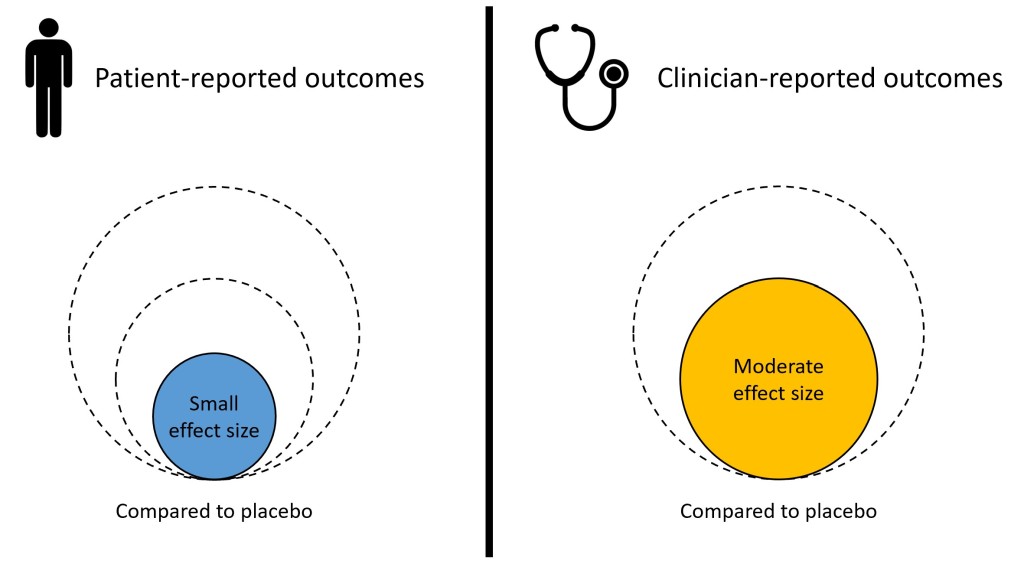
- Patients reported small improvements across all pharmacotherapy (see above) conditions compared to placebo. That is to say, compared to patients who took an inert pill, patients on any of the medication (see above) reported slightly improvements.
- Clinicians reported moderate improvements across all pharmacotherapy conditions compared to placebo. That is to say, when clinicians rated changes in symptom severity, they rated moderate improvements in patients who took any of the medication compared to patients who were on an inert pill (placebo).
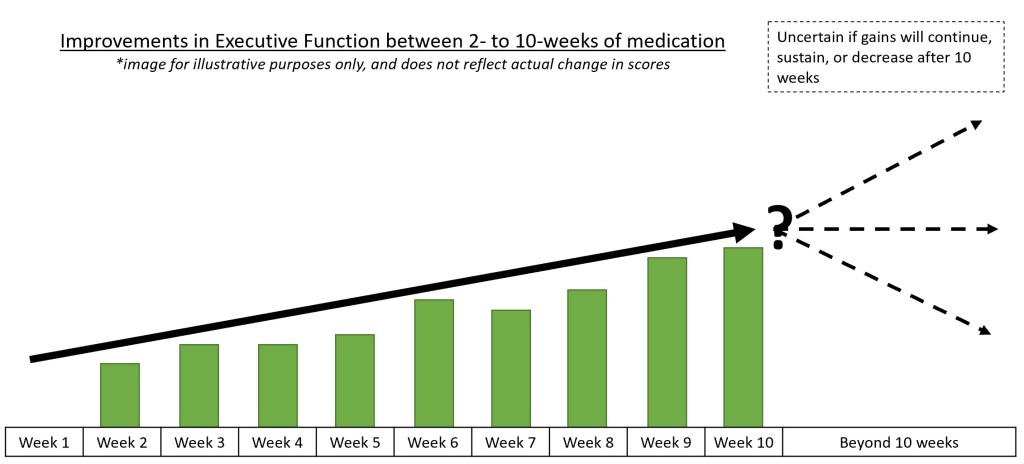
- Studies which examined the impact of pharmacotherapy on executive functioning (measured using the BRIEF-A instrument) reported moderate improvements across treatment. However, these studies did not evaluate if the gains were sustained beyond treatment phase. That is to say, patients who were started on medication showed improvements in their executive functioning between 2- to 10-weeks of medication. We do not have data to know if this improvement continued beyond 10 weeks, sustained beyond 10 weeks, or decreased after 10 weeks. As such, the study suggested that pharmacotherapy had resulted in short-term gains in executive functioning in adults with ADHD.
- Only 5 studies evaluated the impact of atomoxetine on Quality of Life (QoL). It was found that atomoxetine was associated with a slight improvement in the QoL of adults with ADHD. That is to say, adults with ADHD who took atomoxetine reported slightly better QoL compared to adults who took an inert pill. However, as this finding was from a small number of studies (only 5), caution is required when interpreting it due to risk of bias.
- A total of 33 studies evaluated the risk of adverse-events (side effects) of pharmacotherapy compared to placebo. There were no significant differences in the risk of adverse-events across any types of pharmacotherapy (see above). That is to say, taking medication did not result in more side effects than taking an inert pill.
- In 52 studies evaluated, pharmacotherapy was associated with greater risk of study withdrawal as a result of adverse-events. That is to say, adults who took medication and experienced side effects were more likely to withdraw from the studies compared to those who took an inert pill.
Overall, the current meta-analysis has found that ADHD medication was slightly more effective than placebo in improving patient- and clinician-reported outcomes, and was also somewhat effective in improving executive functioning and quality of life. However, the authors also cautioned that how these small to moderate improvements translated into real-world benefits and experiences were unclear. After all, significant changes in questionnaire scores may not always correspond to subjective perception of improvements in daily functioning.
ADHD medication was slightly more effective than placebo in improving patient- and clinician-reported outcomes, and was also somewhat effective in improving executive functioning and quality of life.
It should be noted that while the results appeared positive, the small benefit of medication was made insignificant when the same researchers removed studies with moderate to high risk of bias. That is to say, a small positive benefit of medication was observed when we considered all available studies (biased or not). When only studies of lower bias were included, medication did not outperform placebo. Additionally, when all studies were considered, atomoxetine was superior to other drug therapies. However, this effect was not observed when only studies with low-risk of bias were considered. That is to say, atomoxetine was better than other medication in treating adult ADHD when all studies (biased or not) were considered. However, this apparent superior effect was no longer present when we removed studies with moderate- to high-risk of bias.
Psychosocial Treatment for adults with ADHD
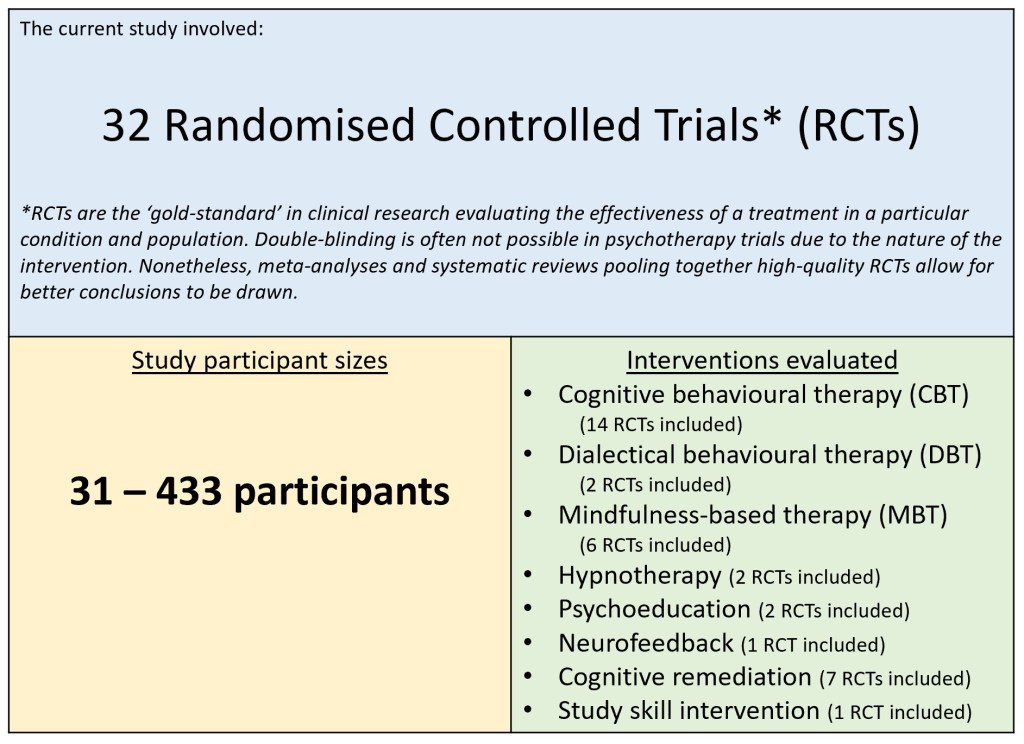
In this study, researchers conducted a systematic review evaluating 32 RCTs that cover 8 different psychosocial treatment for adults with ADHD: cognitive-behavioural therapy (CBT), dialectical behavioural therapy (DBT), mindfulness-based therapy (MBT), hypnotherapy, psychoeducation, neurofeedback, cognitive remediation (e.g. ‘brain training’), and study skill intervention.
Findings:
- In 5 studies, both individual and group CBT were superior to treatment-as-usual (TAU) in reducing ADHD symptoms based on self- or independent-report. However, as the studies were not double-blind, CBT participants might have received more attention than controls.
- CBT was superior to waitlist control in 2 studies.
- CBT was also equal or better than counselling in treating adult ADHD symptoms in 3 studies.
- CBT was better than relaxation training; the improvements were greater, faster, and was sustained at 12-month follow-up. However, as it was the finding of only 1 study, that limited the robustness of the conclusion.

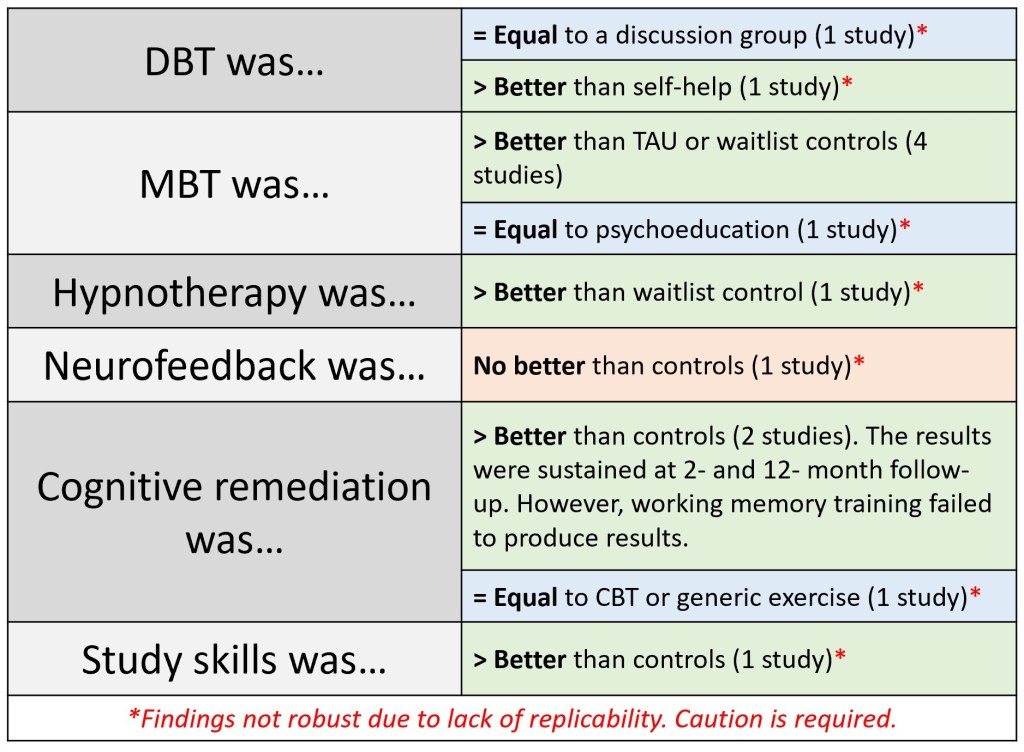
- DBT was comparable to a discussion group, but was superior to self-help in treating ADHD symptoms. However, as the findings were from 1 study each, the results may not be replicable; thus the conclusions are less robust.
- MBT was superior to TAU and waitlist controls in 4 studies, but was comparable to a psychoeducation group (1 study).
- Hypnotherapy was superior to waitlist control in 1 study.
- Neurofeedback was no better than active controls (sham neurofeedback and metacognitive therapy) in 1 study.
- Cognitive remediation was superior to controls in 2 studies, and the results sustained at 2- and 12-month follow-up. However, specific working-memory training failed to produce significant results. Cognitive remediation was also not superior to CBT or generic exercise.
- Study skills intervention (self-monitoring) was better than the control group in improving self-report ADHD symptoms in 1 study. This finding was not replicated, and thus, should be interpreted cautiously.
Overall, the authors concluded that among the various psychosocial interventions, CBT was associated with a reduction in the core behavioural symptoms of ADHD. This finding was supported by a separate meta-analytic study involving 12 studies and 680 participants. In the study by López-Pinar and colleagues (2018), CBT was found to have medium-to-large effect sizes in the treatment of ADHD symptoms. Participants showed significant improvements in inattention, hyperactivity/impulsivity, overall ADHD symptoms, and global functioning compared to a control group. These gains were sustained up to 12-months post-treatment, indicating long-term benefits of CBT in the treatment of ADHD in adults.
In the current systematic review unfortunately, due to a lack of replicability as well as a high risk of bias, robust conclusions cannot be made about the other psychosocial interventions. Nonetheless, it was noted that DBT, MBT, and cognitive remediation were promising treatments. Similar conclusions were made by López-Pinar et al. (2018). In their meta-analysis, while CBT was demonstrably superior to DBT and biofeedback (smaller effect sizes), DBT, MBT, and biofeedback were nonetheless promising treatments with potential to be alternatives to CBT.
In our current review, while CBT had demonstrated significant efficacy in the treatment of adult ADHD, challenges remain. One challenge with psychosocial interventions is the effect of placebo on treatment outcomes. While it is often easy to demonstrate superiority of treatment condition to waitlist or TAU controls (e.g. do something > doing nothing), comparisons with active controls often produce mixed results (e.g. CBT vs counselling). Additionally, due to the inherent nature of psychosocial interventions, it is often difficult to mimic a perfect sham control condition. Therefore, identifying the “active ingredient” remains the challenge, as multiple components go hand-in-hand (e.g. emphatic listening, attention, affirmation, psychoeducation). Perhaps future studies may adopt an additive or dismantling study design to help us better understand the mechanisms of change. Until then, we should avoid overhyping treatment outcomes.
Conclusion
In today’s article, we reviewed 2 separate studies that examined evidence-based treatments for adults with ADHD. From the studies, it would appear that both pharmacotherapy and non-pharmacological (CBT in particular) treatments were efficacious in treating ADHD in adults. Unfortunately, more recent meta-analytic studies or systematic reviews comparing medication to psychosocial interventions could not be found. As such, we do not know if medication is superior, equal, or inferior to non-pharmacological treatments. Having high-quality studies which compare both forms of treatment would definitely allow for better-informed decisions to be made.
Nonetheless, the 2018 guidelines published by the National Institute for Health and Care Excellence (NICE) UK recommended medication as the primary intervention of choice, followed by non-pharmacological treatments if: [1] the person has made an informed choice; [2] the person has difficulties adhering to medication; and [3] medication was ineffective, or not well tolerated. A combination of medication + non-pharmacological treatment was also recommended for adults who have benefitted from medication, but whose symptoms still cause significant impairment.
In the next post, we hope to examine the diagnostic process of ADHD and cover what research-informed diagnostic process is like.
Eugene

One thought on “Research Review: Evidence-based treatments for adults with ADHD”