
Anxiety disorders are a cluster of clinical conditions that affect between 3.8-25.0% of the population (Remes et al., 2016). It was also reported that women, young adults, and persons with chronic diseases were at greater risks of developing anxiety disorders (Remes et al., 2016). In today’s post, we will take a look at what the efficacious treatments for some common anxiety disorders – specifically Generalised Anxiety Disorder (GAD), Panic Disorder (with/without Agoraphobia; PDA), and Social Anxiety Disorder (SAD) – are.
Note: The first and last author of the paper had declared that they were on the speakers’ board for several pharmaceutical companies. As such, there is a risk of bias for pharmacotherapy.
A total of 234 studies involving 37,333 patients were included in the current meta-analysis, making it one of the largest analyses to date. This meant that the conclusions arrived were likely more robust (sans the risk of bias).
Two different types of effect sizes were reported in the study. The first was uncontrolled pre-post treatment effect size. This was essentially the change in anxiety severity observed before and after treatment. However, as it is uncontrolled (e.g. not compared against a placebo or control group), such effect sizes are often overestimated due to the influence of multiple factors (placebo effects being a large one), and would thus not be the focus of this review. The second type of effect size that was reported in the study was ‘active vs control’ effect size. Essentially, the authors compared psychotherapy vs control conditions (waitlist, psychological placebo, placebo pill), or pharmacotherapy vs placebo pill. This will allow us to control for random variables that influence the outcomes, thereby providing a more accurate reflection of a treatment’s true effects. In the rest of this review, we will compare active vs control effect sizes when comparing treatments.
Pharmacotherapy vs placebo
A total of 21 different drug treatments were compared against a placebo pill. Effectiveness of the drugs in the treatment of generalised anxiety, panic disorder, or social anxiety ranged from d = 0.17 – 0.96 (larger is better). Three drugs had non-significant effects: citalopram, moclobemide, and opipramol. This meant that responses to these drugs were not significantly different from placebo. In contrast, the largest effect sizes were found for phenelzine (0.96), clomipramine (0.87), and lorazepam (0.87).

Medications indicated with a * have small study sample sizes, and may thus have higher rates of error
In short, a significant number of medication were found to be relatively efficacious in treating GAD, PDA, and SAD. However, an individual’s response to the medication varies, and consultation with a psychiatrist is warranted to identify the best drug therapy that is well tolerated (side effects taken into consideration).
Psychotherapy vs control
Individual cognitive-behavior therapy (CBT), group CBT, relaxation, and non-face-to-face therapies were compared against waitlist controls, psychological placebo, and drug placebo. Treatment conditions that were compared against a waitlist control had the strongest effect sizes, which was not surprising as it meant doing something (treatment) was superior to doing nothing (waitlist). Individual CBT, group CBT, and relaxation training were the most effective treatments for anxiety compared to waiting.

Of greater interest perhaps is how these treatment performed against a psychological placebo, or a drug placebo. From the study, only CBT conditions (individual and group) had placebo comparisons. Only individual CBT was found to be significantly better than placebo (d = 0.57 & 0.75). Group CBT was not significantly different from drug placebo.

Taken as a whole, in the treatment of generalised anxiety, panic disorder, and social anxiety, all the psychotherapy treatments evaluated were effective compared to waiting (no treatment). Compared against placebo conditions, only individual CBT was shown to be superior.
Psychotherapy vs Pharmacotherapy
Using a drug placebo as a common point of comparison, we could thus see that in the treatment of anxiety disorders, individual CBT was at least as effective as half of the drug therapies available.

Moclobemide, Opipramol, and Citalopram had non-significant effects
While some might interpret the results as medication being superior to psychotherapy in treating anxiety disorders, we should also consider if the side effects of medication are well tolerated by individuals.
“those who had psychotherapy continued to make improvements for 2 years after treatment had ended. Those who took medication experienced a slight worsening of their anxiety symptoms over 2 years after they had stopped medication.”
Of significant interest however, was a meta-analysis of follow-up studies conducted by the same research team on the long term effects of psychotherapy or medication on anxiety. Bandelow and team (2018) found that individuals who had received CBT or other psychotherapy for their anxiety had continued to make progress over the next 2 years (104 weeks) after treatment had ended. In contrast, individuals who had taken medication saw a non-significant decline in their gains after treatment had ended.
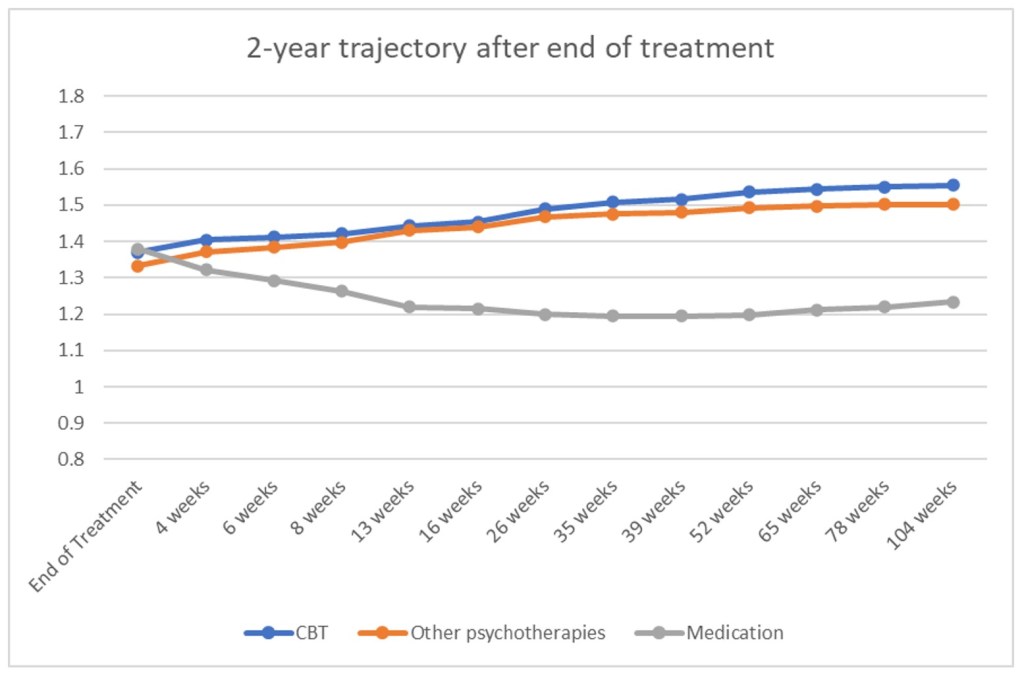
Sloping up = continued improvements; sloping down = decline/worsening
In short, those who had psychotherapy continued to make improvements for 2 years after treatment had ended. Those who took medication experienced a slight (but non-significant) worsening of their anxiety symptoms over 2 years after they had stopped medication.
One possible reason could be how these treatment options bring about their change. In psychotherapy, individuals are taught skills to cope with their anxiety, or are exposed to the stimulus to reduce or extinguish the association between threat appraisal and anxious response. As such, these skills and exposure could continue to support the individual well after treatment has ended. In contrast, medication changes the neurobiology of an individual’s brain by altering the concentration of neurotransmitters involved in the regulation of certain emotions or mood states. Hence, cessation of treatment might result in some worsening of symptoms, albeit slightly.
Conclusion
The current meta-analysis has shown that both medication and psychotherapy (specifically CBT) were efficacious in the treatment of GAD, PDA, and SAD. Both modes of treatment have their costs and benefits, and we should always bring these up for discussion to find the treatment option that best suits our needs and preferences.
Eugene
References:
- Bandelow, B., Sagebiel, A., Belz, M., Görlich, Y., Michaelis, S., & Wedekind, D. (2018). Enduring effects of psychological treatments for anxiety disorders: meta-analysis of follow-up studies. The British Journal of Psychiatry, 1-6. doi: 10.1192/bjp.2018.49
- Remes, O., Brayne, C., van der Linde, R., & Lafortune, L. (2016). A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain and Behavior, 6(7), e00497. doi: 10.1002/brb3.497
