Psychotherapy (or talk therapy) is a divisive topic. To some, it’s a saving grace. To others, it is nothing more than a scam. Efficacy studies on the positive impact of psychotherapy have also been varied. The American Psychiatric Association estimated that up to 75% of individuals who have had psychotherapy benefitted from it. Moritz et al. (2019) reported that up to 95.6% of people with depression who had received psychotherapy experienced positive effects. Others have claimed that while psychotherapy is beneficial as a treatment for mental health conditions, the purported benefits of psychotherapy are overstated (Driessen et al., 2015), as trials showing little to no effects are often unpublished (e.g. file drawer effect). Previous Blue. posts evaluating high-quality evidence (e.g. systematic reviews and meta-analyses) have also shown that psychotherapy can indeed be beneficial in treating a variety of conditions, though effect sizes are generally modest and should not be overstated.
The debate over the effectiveness of psychotherapy is however not the topic of today’s post. Beneficial as it may be, in today’s post, I’d like to share more about a very important but often neglected area in psychotherapy – the experience of negative (or adverse side) effects of psychotherapy.
The Myth that Psychotherapy is Harmless
To some, the reason to consider psychotherapy above other treatment options is in its apparent lack of side effects (Linden & Schermuly-Haupt, 2014). Well, psychotherapy is after all just a process of talking about one’s problems right? What harm could possibly come out of it? Included below are screengrabs of statements made by fellow clinicians.


Unfortunately, like many other effective treatments, psychotherapy does indeed have side effects (termed ‘adverse effects’, ‘negative effects’, or ‘deterioration effects’ in research literature; Berk & Parker, 2009). A recent study by Moritz and colleagues (2019) found that up to 38.5% of individuals with depression who received psychotherapy reported experiencing side effects. Another study by Schermuly-Haupt, Linden, and Rush (2018) reported the presence of at least one side effect in 43% of participants who received Cognitive Behaviour Therapy (CBT). Meditation, a technique frequently used in psychotherapy has also been found to elicit unpleasant experiences (e.g. anxiety, fear, distorted emotions or thoughts) in a quarter of participants (Schlosser et al., 2019), a finding that was replicated in a separate study (Cebolla et al., 2017). A large scale survey involving nearly 15,000 participants in the United Kingdom found that long-lasting negative effects were present among approximately 5% of recipients of psychotherapy regardless of the type of psychotherapy received (CBT, counselling, psychodynamic therapy, cognitive analytical therapy, low-intensity therapy, humanistic therapy, solution-focused therapy) and the delivery (individual or group therapy; Crawford et al., 2016), suggesting that the presence of adverse effects is general across all forms of psychotherapy.
Given the large percentage of reported side effects in psychotherapy and its associated techniques (e.g. exposure, see Meuret et al., 2012), it is concerning that such effects are rarely acknowledged or discussed in clinical settings.
While current numbers are unavailable, the belief that psychotherapy is without side effects is unfortunately a myth endorsed by many clinicians. In a study of psychologists’ knowledge in the United States, Boisvert and Faust (2006) found that up to 28% of practicing psychologists were unaware that psychotherapy can be harmful. That is to say 1 in 4 practicing psychologists reported being unaware of the harms of psychotherapy. Given that the research was published 15 years ago, perhaps we could be hopeful that the field has advanced since. Except that it hasn’t exactly advanced much. Research into the adverse effects of psychotherapy is still severely lacking (Linden & Schermuly-Haupt, 2014; Rozental et al., 2018).
Recognising adverse effects
Perhaps one reason adverse effects are rarely discussed and difficult to research in psychotherapy is due to the difficulties defining and establishing what exactly constitutes it (Linden & Schermuly-Haupt, 2014). After all, many people who seek psychotherapy bring along with them a myriad of psychosocial challenges and symptoms. Clearly identifying and delineating which symptoms are a direct consequence of psychotherapy can be tricky.
To that end, Linden and Schermuly-Haupt (2014) suggested for clinicians to first note down all ‘unwanted events’ that happen in therapy. ‘Unwanted events’ was defined as “events which occur parallel to or in the context of treatment and which are burdensome to the patient and/or his environment, independent of whether they are unavoidable or even necessary to reach a treatment goal.” After which, unwanted events which were likely due to psychotherapy, rated on a probability scale, were considered ‘adverse treatment reactions’. Finally, adverse treatment reactions that were caused by appropriate treatment were labelled ‘side effects’, while adverse treatment reactions that were caused by inappropriate treatment constituted ‘malpractice effects’.
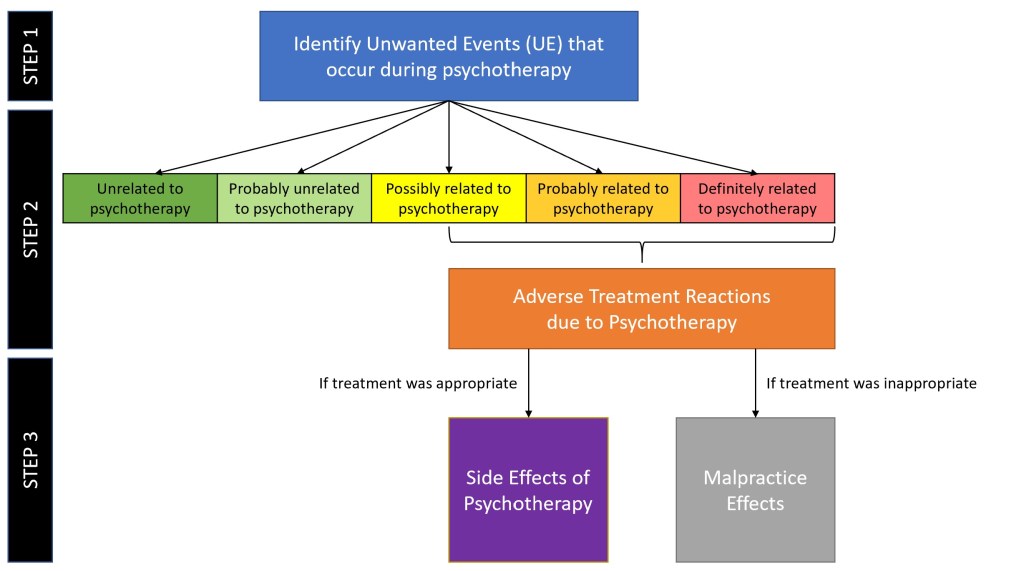
As you can see, side effects/adverse effects of psychotherapy are essentially unintended adverse consequences that occur through the appropriate administration of a treatment.
To help identify adverse effects that may occur during psychotherapy, several tools have been developed. The Positive and Negative Effects of Psychotherapy Scale (PANEPS; Moritz et al., 2019), and the Negative Effects Questionnaire (NEQ; Rozental et al., 2016), are among several tools developed to measure adverse effects of psychotherapy (see Linden & Schermuly-Haupt, 2014 for more). While clinicians often routinely administer scales and tools to measure symptoms and functioning, perhaps it is time for us to also consider administering adjunct tools to concurrently monitor adverse effects over the course of treatment.
The adverse effects of psychotherapy
Emergence of new symptoms
One category of adverse effects due to psychotherapy is the emergence of new symptoms that were absent prior to treatment. In a study conducted by Schneider and colleagues (2020), it was reported that 1 out of 256 clients (0.4%) who had exposure and response prevention (ERP) treatment for obsessive-compulsive disorder (OCD) subsequently developed psychotic symptoms and serious dissociations that required hospitalization. While it was eventually attributed to an undisclosed trauma by the client, the adverse effect was nonetheless brought about by psychotherapy.
When Rozental and colleagues (2019) evaluated data involving 281 study participants, the emergence of new symptoms were found in a sizeable proportion of participants. 15.7% of participants started to feel that their issues could not be made any better, 8.2% of participants became afraid that others would find out about their treatment, 5.3% of participants started feeling shame, 5.0% of participants started to develop a dependency on treatment, and 0.7% started experiencing suicide ideation.
Studies have also found that individuals who had received psychological debriefing following a critical or stressful incident had an increased risk of developing post-traumatic stress symptoms compared to those who did not receive psychological debriefing (Rose et al., 2002; Sijbrandij et al., 2006).
Worsening of existing symptoms
In some situations, psychotherapy could result in the worsening of pre-existing symptoms. In the treatment of OCD using ERP, 1 of 256 clients (0.4%) reported being unable to work for 6 months due to the worsening of their OCD symptoms as a result of treatment (Schneider et al., 2020). In clients who received CBT, 9% reported that their symptoms had worsen due to psychotherapy (Schermuly-Haupt, Linden, & Rush, 2018).
In another study involving 281 participants, 24.6% of participants reported experiencing more anxiety, 23.5% of participants experienced more unpleasant feelings, 15.3% of participants had more problems with sleep, 8.2% of participants felt more hopeless than before, and 8.2% of participants felt like their condition worsened (Rozental et al., 2019).
Adverse impact on social relations
Beyond intrapersonal experiences, adverse effects as a result of psychotherapy can also be interpersonal. In the treatment of depression, 13 of 135 (9.8%) study participants reported that their relationships with family or friends had deteriorated (Moritz et al., 2019). Approximately 6% of individuals who had received CBT also reported strains in family relations following the commencement of psychotherapy (Schermuly-Haupt, Linden, & Rush, 2018). Other adverse effects include changes in relationships at work, in therapy, or in their social network (Schermuly-Haupt, Linden, & Rush, 2018).
Negative wellbeing
The last category of adverse effects is negative wellbeing, which may in fact be the overall feeling brought about by both intra- and interpersonal adverse effects. In a study involving 100 participants receiving CBT, Schermuly-Haupt, Linden, and Rush (2018) found that 27% of participants reported negative wellbeing as a result of psychotherapy.
What then?
Thus far we have seen how psychotherapy is not without adverse effects. In fact, those adverse effects such as developing new symptoms, worsening of existing symptoms, negative impact on social relationships and on overall wellbeing can affect up to approximately 40% of individuals undergoing psychotherapy.
The good news is as frightening as it may sound, adverse effects of psychotherapy can actually be managed, treated, and resolved over the course of treatment. The vast majority of adverse effects are mild to moderate in severity, and may resolve in days (Schermuly-Haupt, Linden, & Rush, 2018). It gets trickier when a client experiencing adverse effects arrive at the conclusion that psychotherapy is not working, and terminate treatment prematurely. This premature termination prevents the resolution of those adverse effects, leaving the client worse off than before. That is why it is important for clinicians to share, and for clients to be aware, that adverse effects can and do occur in psychotherapy, so that the number of incidents of premature termination could be reduced when clients experience these effects.
With all that has been said, I remain hopeful. Through this article, I hope that along with the other emerging voices speaking up on the topic, more clinicians and clients will be cognizant of the risks of psychotherapy. In fact, a quick search using the terms ‘adverse’ + ‘negative’ + ‘effects’ + ‘psychotherapy’ on Google brought about multiple hits on the front page, perhaps suggesting greater recognition of it.
Having said that, more can definitely be done in this area. For a start:
- Psychologists, psychiatrists, counsellors, and psychotherapists need to learn about and acknowledge the risks of psychotherapy, and reject the myth that psychotherapy is without harm;
- Clinicians should actively inform and discuss the risk of adverse effects from psychotherapy with their clients, the same way that side effects of medication are discussed with clients;
- Clinicians can also consider using one of the several tools developed to measure adverse effects as an adjunct to progress monitoring;
- Clients who experience adverse effects of psychotherapy should bring up the matter to their therapist instead of terminating treatment prematurely
I hope that in the years to come, there will be better recognition of the adverse effects of psychotherapy. Along with that, I hope that more research in this area will also be done. Only by recognizing an issue, can we endeavour to do better to address it. Only by doing so, can we truly act in the best interest of our clients.
Eugene
References:
- Berk, M., & Parker, G. (2009). The Elephant on the Couch: Side-Effects of Psychotherapy. Australian & New Zealand Journal of Psychiatry, 43, 787-794.
- Boisvert, C. M., & Faust, D. (2006). Practicing psychologists’ knowledge of general psychotherapy research findings: Implications for science-practice relations. Professional Psychology: Research and Practice, 37(6), 708–716.
- Cebolla, A., Demarzo, M., Martins, P., Soler, J., Garcia-Campayo, J. (2017). Unwanted effects: Is there a negative side of meditation? A multicentre survey. PLoS ONE, 12(9): e0183137.
- Crawford, M. J., Thana, L., Farquharson, L., Palmer, L., … & Parry, G. D. (2016). Patient experience of negative effects of psychological treatment: results of a national survey. The British Journal of Psychiatry, 208, 260–265. doi: 10.1192/bjp.bp.114.162628
- Driessen, E., Hollon, S. D., Bockting, C. L. H., Cuijpers, P., & Turner, E. H. (2015). Does Publication Bias Inflate the Apparent Efficacy of Psychological Treatment for Major Depressive Disorder? A Systematic Review and Meta-Analysis of US National Institutes of Health-Funded Trials. PLoS One, 10(9):e0137864. doi: 10.1371/journal.pone.0137864
- Linden, M., & Schermuly-Haupt, M.-L. (2014). Definition, assessment and rate of psychotherapy side effects. World Psychiatry, 13(3), 306-309.
- Meuret, A. E., Seidel, A., Rosenfield, B., Hofmann, S. G., & Rosenfield, D. (2012). Does fear reactivity during exposure predict panic symptom reduction? Journal of Consulting and Clinical Psychology, 80(5), 773-785.
- Moritz, S., Nestoriuc, Y., Rief, W., Klein, J. P., … & Peth, J. (2019). It can’t hurt, right? Adverse effects of psychotherapy in patients with depression. European Archives of Psychiatry and Clinical Neuroscience, 269(5), 577-586.
- Rose, S., Bisson, J. , Churchill R., & Wessely, S. (2002). Psychological debriefing for preventing post traumatic stress disorder (PTSD). The Cochrane Database of Systematic Reviews, 2:CD000560. doi: 10.1002/14651858.CD000560
- Rozental, A., Castonguay, L., Dimidjian, S., Lambert, M., … & Carlbring, P. (2018). Negative effects in psychotherapy: commentary and recommendations for future research and clinical practice. BJPsych Open, 4(4), 307-312.
- Rozental, A., Kottorp, A., Boettcher, J., Andersson, G., & Carlbring, P. (2016). Negative effects of psychological treatments: An exploratory factor analysis of the Negative Effects Questionnaire for monitoring and reporting adverse and unwanted events. PLoS One, 11, e0157503. doi: https://doi.org/10.1371/journal.pone.0157503
- Schermuly-Haupt, M.-L., Linden, M., & Rush, A. J. (2018). Unwanted Events and Side Effects in Cognitive Behavior Therapy. Cognitive Therapy and Research, 42, 219–229
- Schlosser, M., Sparby, T., Voros, S., Jones, R., & Marchant, N. L. (2019). Unpleasant meditation-related experiences in regular meditators: prevalence, predictors, and conceptual considerations. PLoS ONE, 14(5): e0216643
- Schneider, S. C., Knott, L., Cepeda, S. L., Hana, L. M., … Storch, E. A. (2020). Serious negative consequences associated with exposure and response prevention for obsessive‐compulsive disorder: A survey of therapist attitudes and experiences. Depression and Anxiety, 37(5), 418-428.
- Sijbrandij, M., Olff, M., Reitsma, J. B., Carlier, I. V. E., & Gersons, B. P. R. (2006). Emotional or education debriefing after psychological trauma. Randomised controlled trial. The British Journal of Psychiatry, 189, 150-155.

2 thoughts on “Opinion/Commentary: When help harms – the unintended adverse effects of psychotherapy”