
Note: a newer article on the subject was posted on 11/05/2024.
Recently, I was on the Internet when a rant in an online forum caught my attention. It was from a supposed psychotherapist who was currently undergoing therapy themselves (gender neutral). In it, they shared their exasperation with CBT and positive psychology, going on about how ‘CBT invalidates people’s feelings by reducing it to their thoughts’, and how ‘telling people to think positively will not work as they are in poverty, abusive relationships, homelessness etc.’
Commenters on the thread soon started sharing their personal horror stories with CBT one after another. Their comments could be largely categorized into two broad themes: practitioners who felt like CBT has an extremely narrow scope that only works for select individuals and would rather defer to other therapeutic modalities like psychodynamic therapy; and recipients of CBT who felt like they were not heard, but was instead “having theory forced down [their] throat[s]”.
These two broad categories of criticisms of CBT are not unheard of. Over the years, I’ve heard psychiatrists, social workers, and occupational therapists tell me that “CBT doesn’t work”, “it is not flexible”, “I tell my patients to think positive”, “just follow the manual right?”
Now, CBT does not work for everyone. That is something that we would all need to acknowledge. Multiple reasons may explain this, such as personal preferences (Lindhiem et al., 2014), past negative experiences with CBT, or the type of psychopathology (Hofmann et al., 2012). With that out of the way, what stood out for me from the above however, was how practitioners and clients of CBT appeared to have (mis)understood what it is. Many people think that they understand CBT. Perhaps some do. But in the examples above, none of them appeared to fully grasp it. Neither have I. Learning CBT is always a work-in-progress, and I’ll get to it in the later sections.
In my opinion, this misconception of CBT can be attributed to a few reasons.
First, the popularity of CBT as an evidence-based treatment for a variety of mental health conditions has resulted in its rapid commercialization and proliferation. Search ‘cognitive behaviour therapy training’ online and one would find a plethora of purported CBT training courses – some by independent trainers, some by small organisations, and some by larger institutions. Unfortunately, as with the commercialization of many things, quality control becomes an issue. Not all training programmes are created equal. Some are rigorous, some aren’t. Some are comprehensive, some aren’t. Some are intended to train practitioners of CBT, while others are meant to be samplers, from which more intensive training would follow should one intend to practice CBT formally. In fact, one could easily find many courses online promising “certified CBT training”, only to under-deliver on quality. Many of those courses do not even have a practical component to them. I have had personal experiences from friends who after attending one of these courses, started proclaiming themselves CBT-trained therapists. These quick training programmes may have saturated the therapy space with eager and enthusiastic CBT practitioners, some knowing little more than a diagram.
Next, many post-graduate training courses with CBT component focus a lot on the research literature surrounding CBT efficacy in a variety of treatment conditions, and less on explicitly teaching how to do CBT as a technical skill. Many programmes relegate such technical training to the internship/placement component of the course, where supervisees learn those skills on-the-job from their supervisors. This variability in training (supervisor dependent) results in different trainees picking up different skills from different supervisors. Learning on-the-job is also influenced by the different client populations seen, or where the trainee learns and practices at (outpatient vs inpatient care; chronic vs acute care; specialist vs generalist clinics). In my personal journey as a therapist, I would attribute the honing of my CBT skills less to what I had learnt in my post-graduate training programme, and more to my own professional development after being registered.
When we have practitioners with perhaps less than desired levels of competency practicing ‘CBT’ in various services, that might explain some of the complaints brought about by clients in the examples given above – feeling invalidated, feeling that they weren’t heard, that they’re being told to think positively, or having knowledge forced on them when they may perhaps want to talk about their experiences. Having been a novice therapist practicing CBT, I know this for a fact. My skills (or lack thereof) have affected my clients in more ways than I would have liked. Of course, client factors do also play a part in therapy too. Nonetheless, if we find clients possibly misunderstanding what we teach, or what our therapeutic modality is about, it is the duty of the therapist to correct that misunderstanding (gently and in a non-confrontational manner of course) and to ensure what we teach is pegged at the appropriate level.
In the ensuing paragraphs, I’ll try my best to share what my current understanding of CBT is. I am by no means an expert on CBT, and what I will share is simply based on what I know and have learnt.
Note: The focus of this article will solely be on what CBT is, and isn’t. It will not address issues of efficacy, nor make comparisons to other forms of psychotherapy.
What is CBT?
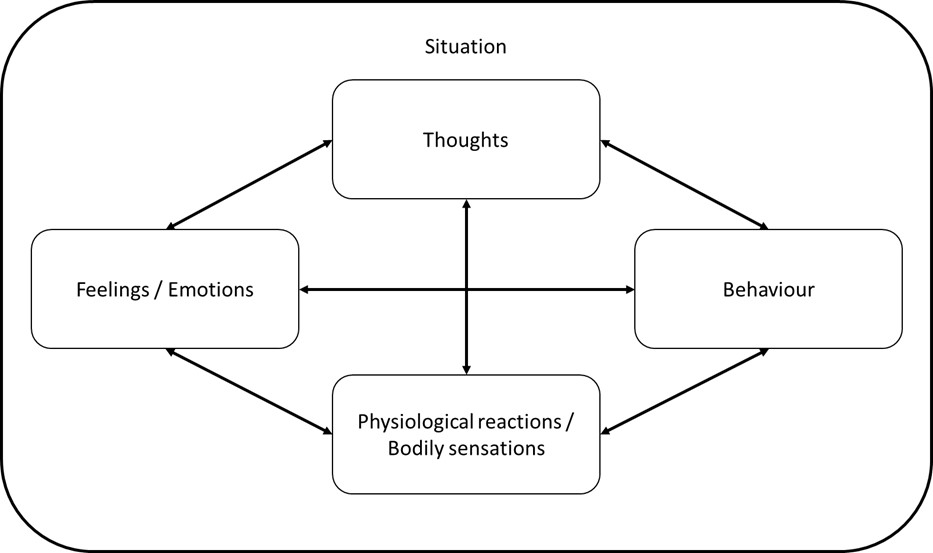
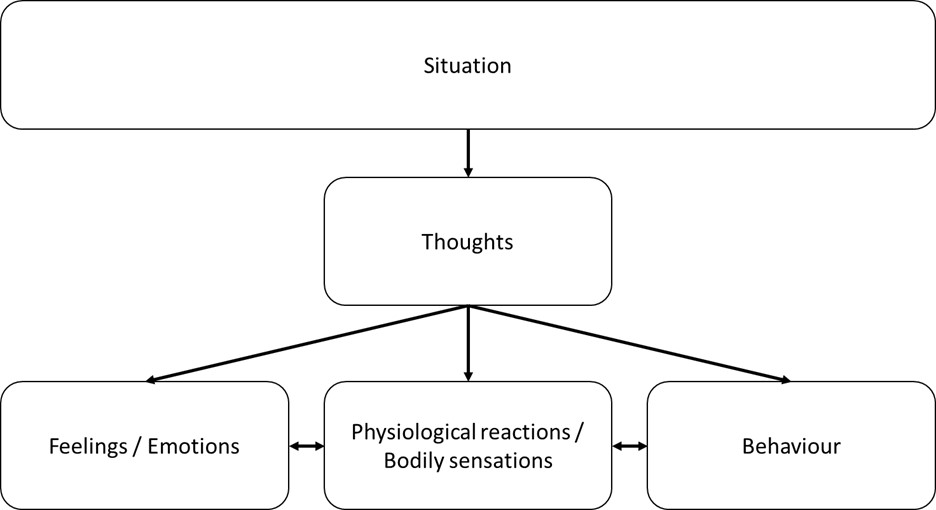
The images above go by several different names: “hot-cross bun” model, 5-part model, cognitive-model, cross-sectional model etc.
So what exactly is CBT? To some, the models above are CBT. An image search on Google with the terms ‘cognitive + behavior + therapy’ would bring you many extremely simplified images illustrating CBT, the most common of them showing the “cognitive triangle” or ”CBT triad”, where CBT is in the middle, encapsulated by interlinked thoughts, feelings, and behaviour. I once had an interaction with a friend that went something like this:
Friend: I saw a patient today and did CBT.
Me: Oh, tell me more.
Friend: I drew out a model and explained to her that her thoughts cause her to feel or behave in a certain way. And that she should change her thoughts by thinking positively.
That, however, is an oversimplification of what CBT is. I think one of the greatest advantages of CBT – the use of simple visual models to explain cognitive conceptualization – is also perhaps one of its biggest weaknesses when people equate CBT as a therapeutic modality to nothing more than the commonly used model. From my experience, this misunderstanding of CBT is unfortunately quite prevalent among many clinicians across different occupations (psychiatrists, doctors, social workers, allied health professionals, psychologists).
Quoting from Judith S. Beck’s “Cognitive Behavior Therapy: Basics and Beyond, Third Edition” book (2021, p.3 & 4), “In all forms of CBT that are derived from Beck’s model, clinicians base treatment on a cognitive formulation: the maladaptive beliefs, behavioral strategies, and maintaining factors that characterize a specific disorder. … the cognitive model proposes that dysfunctional thinking (which influences the client’s mood and behavior) is common to all psychological disturbances. When people learn to evaluate their thinking in a more realistic and adaptive way, they experience a decrease in negative emotion and maladaptive behavior.”
Note how there was no mention that our thoughts cause us to feel or behave in a certain way, nor was there any mention of CBT getting people to think more positively. Rather, dysfunctional thinking or maladaptive beliefs seem to be the common factor that cuts across multiple psychological disturbances, and getting people to look at their thoughts more realistically may alleviate some of that resulting discomfort. At its crux, CBT recognizes that people do have real-world challenges (maintaining factors). To cope with these challenges, people often develop strategies which may or may not be helpful (behavioural strategies). Both real-world challenges and unhelpful coping strategies are things that may need to be resolved. Additionally, prolonged exposure to those challenges and use of unhelpful coping strategies may also reinforce unhelpful beliefs about oneself (maladaptive beliefs). These beliefs may lead to negative/unrealistic automatic thoughts, which may,
- result in prolonged distress even if our real-world challenges are resolved;
- perpetuate use of unhelpful coping strategies that maintain those real-world challenges;
- become obstacles that prevent us from solving those real-world challenges. It is therefore crucial to address all the various aspects in treatment, not just the thoughts.
Let us take a look at an example. If someone is homeless, unemployed, and depressed as a result, CBT isn’t about asking the person to change their thoughts. That does little to address the maintaining factors and is a poor application of a CBT technique. If homelessness and unemployment are factors maintaining the person’s depression, those real-world challenges will need to be targeted. A CBT therapist might start with problem-solving: What are the options available to address homelessness and unemployment? What concrete action plans can the person take? At times, prolonged exposure to unfortunate circumstances and stressors (in this situation homelessness and unemployment) may have resulted in maladaptive beliefs about self (e.g. “I’m worthless”, “I cannot do anything right”), and these might be uncovered in the process of problem-solving. Sometimes they do not affect problem-solving and that is fine. At other times, these beliefs might present as obstacles stopping the person from seeking help at the relevant support agencies. So while we might have started therapy with a focus on solving the practical aspects of someone’s life (homelessness or unemployment), maladaptive beliefs and the associated unhelpful thinking patterns or negative automatic thoughts may present as obstacles that hinder progress on that front. At this point, it is important to address these cognitions through the use of a variety of techniques (see below). Successful navigation of these cognitions may address the obstacles that had prevented appropriate problem-solving, allowing us to once again solve practical problems. This act of solving the maintaining factors might also bring about a positive feedback loop: the person now feels more empowered and hopeful as they have a job or temporary housing, which reinforces adaptive beliefs about self, and further motivates more appropriate behaviours.
As you can see, CBT is more than just ‘thoughts influence feelings and behaviours’. Based on my personal understanding, a general CBT conceptualization might look something like this:
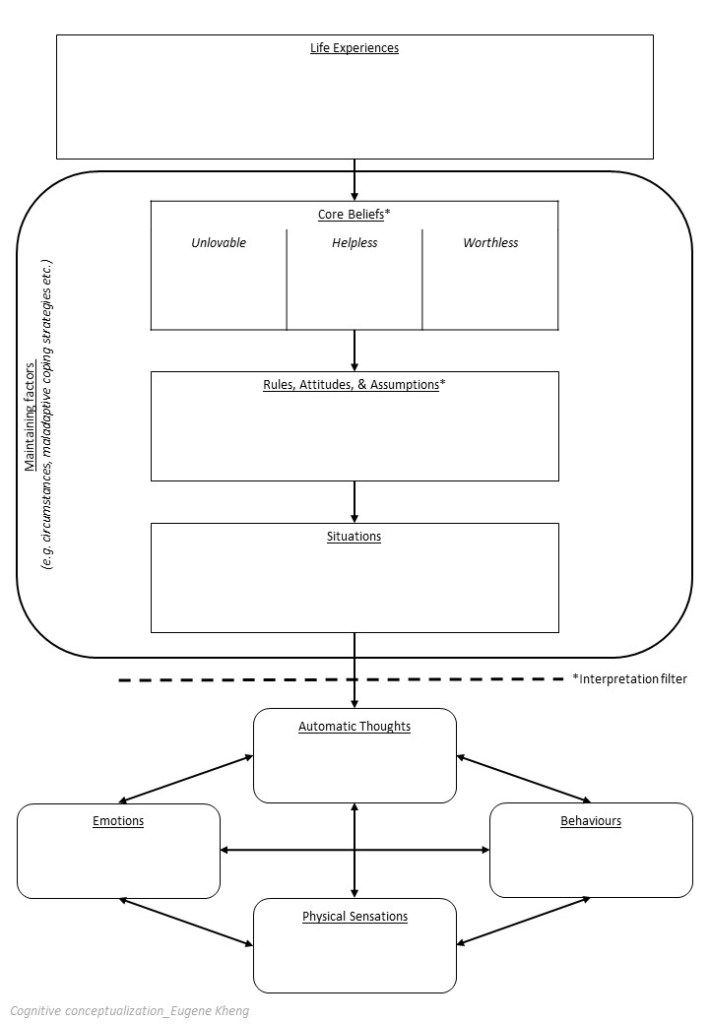
As some might have noticed, a conceptualization model like this would also correspond quite neatly to the commonly used 4Ps (Predisposing, Precipitating, Perpetuating, Protective) model. However, depending on what conditions are being examined, conceptualizations may differ. One could take a look at the various examples in David H. Barlow’s “Clinical Handbook of Psychological Disorders” (2014) to get a sense of how varied conceptualizations can be.
The elegance of CBT is in its seemingly simple concept that accounts for the complex interplay of factors. A skilled therapist will need to formulate accurately in order to know which factors to target at the right time for optimal recovery.
What CBT is Not
Having roughly explained what CBT is, let us now take a look at what some common misconceptions of CBT are and address them. I will be drawing upon heavily from the latest edition of Judith Beck’s “Cognitive Behavior Therapy: Basics and Beyond, Third Edition” (2021) in the process.
Misconception: CBT is rigid and manualized. Practitioners follow standardized protocols.
The very first time I had personally encountered this was when I was a trainee, and a psychiatrist friend of mine made an offhand remark following his sharing about his psychodynamic training. He said, “Oh so as a psychologist, you practice manualized CBT?”
This misunderstanding is not uncommon. I reckon it might be the way CBT as a treatment modality has been studied and evaluated. In research studies, CBT treatment conditions are almost always manualized. In the context of a highly systematic RCT controlling for variables, that would make perfect sense. While manualized CBT programmes are a great way to run time-limited treatment programmes, or CBT groups, individualized CBT therapy accords way more flexibility than given credit for.
According to Basics and Beyond (Beck, 2021), principle 4 of CBT states: “CBT is culturally adapted and tailors treatment to the individual”. Far from being manualized, CBT stresses the importance of taking into account individual differences such as “age, religious or spiritual orientation, ethnicity, socioeconomic status, disability, gender, sexual identity, and sexual orientation” (p.19) in treatment.
Principle 14 states: “CBT uses a variety of techniques to change thinking, mood, and behavior”. Beck (2021, p.24) further explains, “In fact, we adapt strategies from many psychotherapeutic modalities within the context of the cognitive framework. For example, … techniques from acceptance and commitment therapy, behavior therapy, compassion-focused psychotherapy, dialectical behavior therapy, Gestalt therapy, interpersonal psychotherapy, meta-cognitive therapy, mindfulness-based cognitive therapy, person-centered psychotherapy, psychodynamic psychotherapy, schema therapy, solution-based therapy, well-being therapy, or others.”
Give that the above were written by Judith Beck herself, one would find it hard to argue that CBT is highly manualized, or rigid. CBT isn’t the sum of its component techniques. It is a theory, model, and explanation of what precipitates and perpetuates psychological distress. It accords flexibility in addressing those challenges using a variety of techniques from other psychotherapies, within the cognitive framework.
In fact, practitioners who focuses too much on the thought aspect of CBT often miss the forest for the trees. The following are a non-exhaustive list of CBT techniques (from Beck, 2021; and Hayes & Hoffman, 2018) that show great promise when used appropriately to address the relevant challenges:
- Imagery
- Skills training
- Task analysis
- Contingency management
- Stimulus control
- Shaping
- Self-management
- Arousal reduction
- Coping and emotional regulation
- Problem solving
- Exposure strategies
- Behavioral activation
- Interpersonal skills
- Cognitive reappraisal
- Modifying core beliefs
- Cognitive defusion
- Psychological acceptance
- Values-driven approaches
- Mindfulness
- Motivation enhancing techniques
- Crisis management techniques
Misconception: CBT invalidates feelings by focusing on thoughts
This point might have less to do with the therapeutic modality, and more to do with the clinician. At times, overly eager therapists might find themselves spending far too much time focusing on addressing the cognitive components in their clients, neglecting the process of therapy. By process, I mean what goes on in the session between therapist and client. Therapeutic relationship and rapport are examples.
Principle 2 of CBT states: “CBT requires sound therapeutic relationship”. Like in all the other therapeutic modalities, therapist-client rapport is important in CBT. A skilled CBT practitioner is one who is attuned to the emotional aspects of their clients, acknowledging and validating the presence of these feelings. Beck (2021, p.58-69) explains, “In CBT, the Rogerian counseling skills of empathy, genuineness, and positive regard are especially important. You will continuously demonstrate your commitment to and understanding of clients through your empathic statements, choice of words, tone of voice, facial expressions, and body language.” In fact, these counseling skills to attune and validate clients’ emotions are considered prerequisite skills to practicing CBT (or other therapeutic modalities). The challenge for therapists then is to masterfully balance between working on cognitive distortions while not coming across as dismissive or invalidating of one’s emotional experiences.
Misconception: CBT focuses excessively on addressing negative or unhelpful thoughts
There are some truths to this statement. In the past, CBT was focused predominantly on identifying dysfunctional cognitions and addressing them. It is hoped that through the mechanism of restructuring someone’s thoughts and beliefs, improvements to their overall wellbeing and functioning would follow.
However, CBT is not static. It didn’t stay the same as it was when Aaron Beck first conceptualized it in the 1960s. It also didn’t stay the same as it was when the second edition of Basics and Beyond was published (Beck, 2011). In some sense, it is heartening to know that CBT as a modality is constantly evolving based on current scientific research findings. This process of refining and incorporating new and relevant aspects has kept CBT grounded in research evidence. Over the last decade (ref. Basics and Beyond Third Edition by Beck, 2021), CBT has taken on a new paradigm shift that in my opinion might have been influenced by the values-driven approach of Acceptance and Commitment Therapy (ACT). CBT is now recovery-oriented – moving away from its excessive focus on maladaptive cognitions, to focusing on removing hurdles that prevents people from achieving specific goals and valued outcomes.
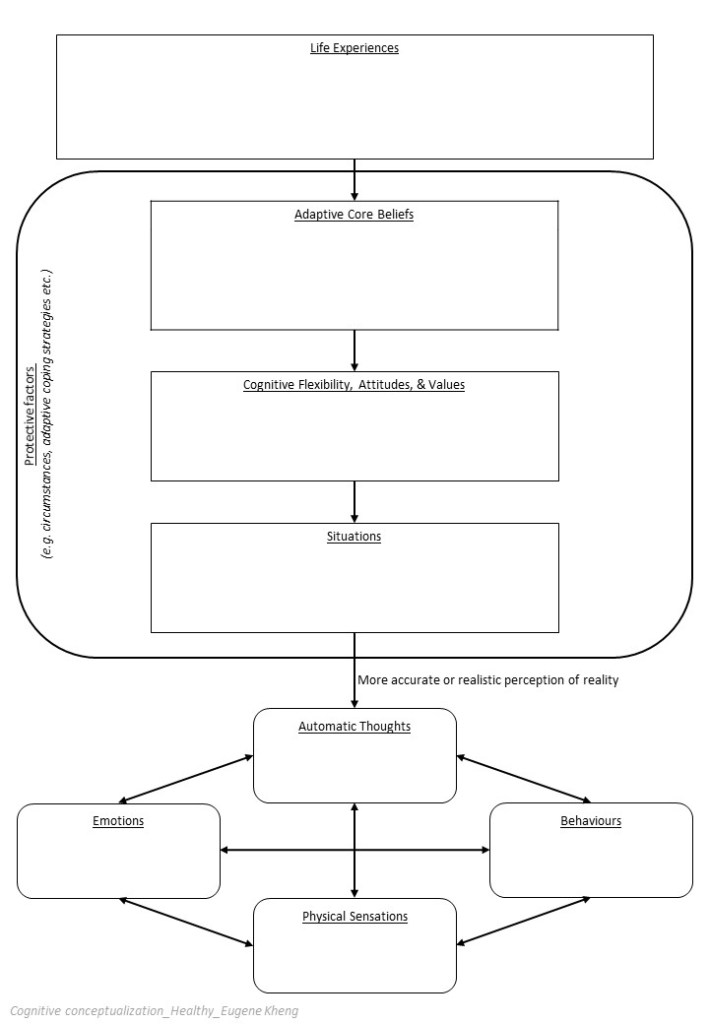
Principle 5 of CBT states: “CBT emphasizes the positive”. While unhelpful thinking patterns are still essential to address, emphasizing positives meant noticing strengths and helpful patterns in people, bringing it up to the table for discussion, and reinforcing those. It is theorized that merely reducing unhelpful thinking styles will not sufficiently address self-perception if we do not concurrently raise and reinforce positive world views, experiences, and thoughts.
Principle 7 of CBT states: “CBT is aspirational, values based, and goal oriented”. As mentioned in brief earlier, recovery-oriented CBT emphasizes goals and values, asking clients to imagine how recovery would look like, and taking deliberate and active steps in that direction. Potential obstacles that may hinder these small steps are considered, and resolved as best as possible. When each small step is successfully taken, additional emphasis is given on these positive experiences, reinforcing them and through that process, build up a more helpful self-perception.
Hence, in recovery-oriented CBT, a strength- and values-focused conceptualization might look something like this:
Misconception: CBT focuses only on the present, but doesn’t help me understand my past
The way CBT sessions are structured may inadvertently give rise to the impression that it focuses only on the present. There is no smoke without fire. This idea may be accurate to a certain degree. CBT does focus fairly strongly on the present. In recovery-oriented CBT, the focus might in fact be on the present (where you are now), and the future (where you want to be). However, that does not mean exploration of the past is beyond the model of CBT.
Principle 8 of CBT states: “CBT initially emphasizes the present”. The key word is ‘initially’. There are practical reasons as to why CBT starts off focusing on the present. Remember how maintaining factors are an essential aspect of CBT’s conceptualization? CBT seeks to identify and address factors that maintain distress, many of which are relevant in the here and now (e.g. poor relationship with peers, doing badly academically, going through a divorce, loss of job). Through that process, it is hoped that clients will have a better understanding of what is happening in their lives right now that maintains their difficulties, but it also familiarizes clients to thinking about their challenges in a certain way, which might be achieved through psychoeducation (Principle 9: “CBT is educative”).
Beck (2021, p.20) identifies three different circumstances in which a CBT therapist might shift the focus to the past, and they are:
- “When the client expresses a strong desire to do so,
- When work directed toward current problems and future aspirations produces insufficient change, or
- When [the therapist] judge[s] that it is important for [the therapist] and clients to understand how and when their key dysfunctional ideas and behavioral coping strategies originated and became maintained.”
As you can see, CBT does not focus only on the present (or future). There is room for clients to work on and make sense of their history. What is important is for the therapist and client to be in agreement and understand the rationale for doing so. After all, if a client is able to make sufficient gains by focusing on the present and future, and does not feel the need to evaluate their past, why spend time and money (by having more sessions) doing so?
Closing
At this point, I hope that you will have a better understanding of what CBT is. In short, CBT is a dynamic (not psychodynamic) therapeutic modality that on the surface may appear deceptively simple. Its apparent simplicity is its strength, but also a weakness when misunderstood by clients and practitioners alike. Digging deeper, we find that far from the common misconceptions raised, CBT is flexible, practical, individualizable, empathetic, and ever evolving. In recovery-orientation, it has shifted its focus away from only evaluating the negative cognitive processes, to reinforcing positive cognitive, emotional, and behavioural aspects, and outcomes. While CBT might focus more on the present and future in the initial stages of treatment, there is plenty of room for therapists and clients to explore past experiences if necessary.
Eugene
For those interested in reading more about CBT, I would highly recommend:
- “Cognitive Behavior Therapy: Basics and Beyond (3rd ed.)” by J. S. Beck (2021),
- “Process-Based CBT: The Science and Core Clinical Competencies of Cognitive Behavioral Therapy” by Hayes & Hofmann (2018), and
- “Recovery-Oriented Cognitive Therapy for Serious Mental Health Conditions” by Beck, Grant, Inverso, Brinen, & Perivoliotis (2021).
PS: The author is a practitioner of multiple therapeutic modalities, and has no conflict of interest to declare.
References
- Barlow, D. H., Beck, A. T., Beutler, L. E., Bleiberg, K. L., & Christensen, A. (Eds.). (2014). Clinical Handbook of Psychological Disorders: A Step-by-Step Treatment Manual (5th ed.). Guilford Publications.
- Beck, J. S. (2021). Cognitive Behavior Therapy: Basics and Beyond (3rd ed.). Guilford Press.
- Beck, J. S. (2011). Cognitive Behavior Therapy: Basics and Beyond (2nd ed.). Guilford Press.
- Hayes, S. C., & Hofmann, S. G. (Eds.). (2018). Process-Based CBT: The Science and Core Clinical Competencies of Cognitive Behavioral Therapy. New Harbinger Publications.
- Hofmann, S. G., Asnaani, A., Vonk, I. J. J., Sawyer, A. T., & Fang, A. (2012). The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cognitive Therapy and Research, 36(5), 427-440.
- Lindhiem, O., Bennett, C. B., Trentacosta, C. J., & McLear, C. (2014). Client preferences affect treatment satisfaction, completion, and clinical outcome: A meta-analysis. Clinical Psychology Review, 24(6), 506-517.

This is indeed a great post. It is important to acknowledge the misunderstanding. Thank you so much.
LikeLike