
In today’s Wassup’ post, we examine a very comprehensive systematic review (396 pages in total) funded by the National Institute for Health Research (NIHR) in the UK to evaluate efficacious and cost effective treatments for OCD. A greater emphasis will be placed on examining the effectiveness of the various interventions, as the costs identified in the study were based on UK healthcare costs, and may therefore restrict generalizability (i.e. may not be as applicable where you are).
In their systematic review, the authors evaluated a sizeable 86 studies comprising 8611 participants, of which 7306 participants in 64 studies were adults, while 1305 participants in 22 studies were children and adolescents.
The Yale-Brown Obsessive-Compulsive Scale (YBOCS) and Children’s YBOCS were the instruments used in the studies to determine treatment effectiveness. The YBOCS and Children’s YBOCS are tools that measure the severity of one’s OCD. As such, changes in YBOCS scores generally indicate improvements or worsening of one’s OCD symptomatology. Hence, effective treatments are those that should result in improvements in YBOCS scores, while the reverse would suggest ineffective, or possibly detrimental treatments.
In their review, the authors compared the following interventions against a placebo control (inactive pill) to determine their effectiveness:
- Medication (SSRIs: Selective Serotonin Reuptake Inhibitors, Venlafaxine, Clomipramine)
- Behaviour Therapy (BT), which includes Exposure and Response Prevention (ERP) as a main component. ERP involves exposing clients to their feared stimuli while preventing their compulsive behaviours, which usually functions as a safety response to their obsessions/fears
- Cognitive Therapy (CT), a talk-therapy based on the cognitive model
- Cognitive Behavioural Therapy (CBT), a talk-therapy based on the cognitive-behavioural model. CBT is typically seen as the extension of CT in which behavioural elements such as behaviour activation, behavioural experimentation, and exposure are included
- Psychotherapy (BT, CT, CBT) in combination with Medication
- Psychological Placebo, which was defined by the study as non-specific psychotherapy, which could include supportive counseling
The reason a placebo condition was included as the control was to account for placebo effects. Effective treatments are thus those that show benefits above and beyond those obtained in the placebo condition. For example, if a participant in the placebo condition made an improvement of 5 points, while a participant in the intervention condition made an improvement of 7 points, the intervention will therefore be considered to have a comparative effectiveness of 7 – 5 = 2 points (superior to placebo). This would imply that the treatment effects observed were likely due to the intervention.
Conversely, if the placebo condition had an improvement of 5 points while the intervention condition only had an improvement of 3 points, the intervention condition will be said to have a comparative effectiveness of 3 – 5 = -2 points (worse than placebo), which may suggest that the treatment is ineffective.
So how did the interventions perform?
When evaluating the different treatment conditions in adults, the authors found that all interventions evaluated were superior to placebo (set at the baseline of ‘0’).
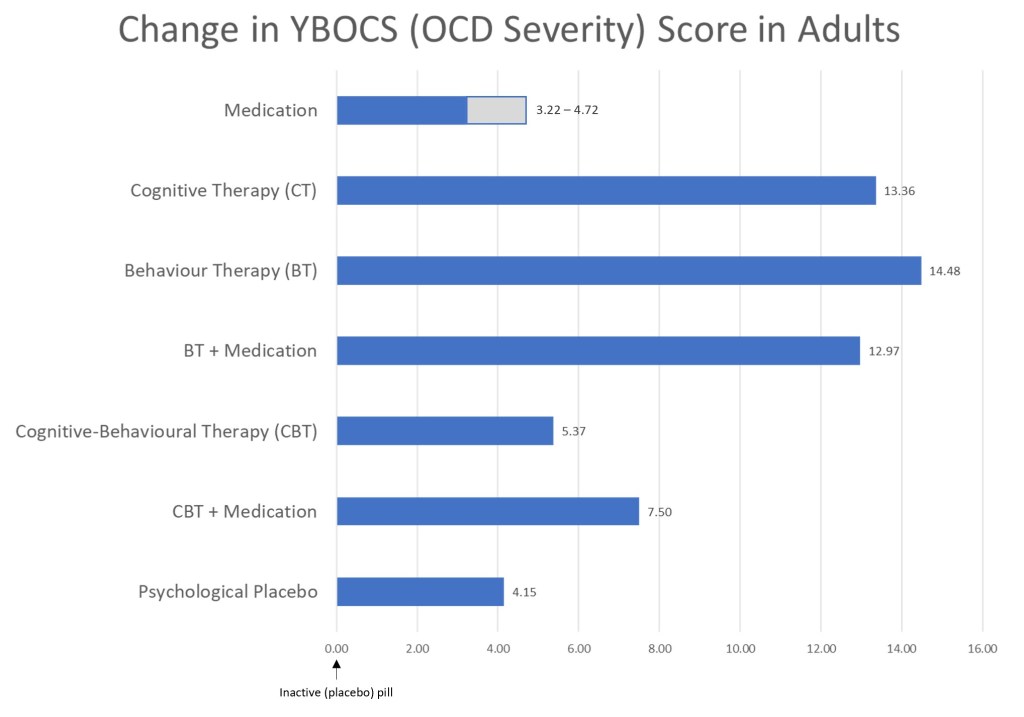
In treating OCD in adults, behaviour therapy (exposure and response prevention) and cognitive therapy were found to be the most efficacious. Surprisingly, cognitive-behavioural therapy only performed slightly better than psychological placebo, and performed significantly poorer than BT and CT. This was despite CBT being the amalgamation of both BT and CT. One possible explanation was study attrition which skewed the results. When the authors took into account attrition effects (e.g. the impact of participants dropping out of the study midway), CBT became as effective as BT and CT in treating OCD. Depending on the type of medication evaluated, the effectiveness in adults varied. Hence, the impact of medication is shown as a range.
Similar to the treatment of OCD in adults, all evaluated interventions in children and adolescents were superior to placebo (baseline score of ‘0’).
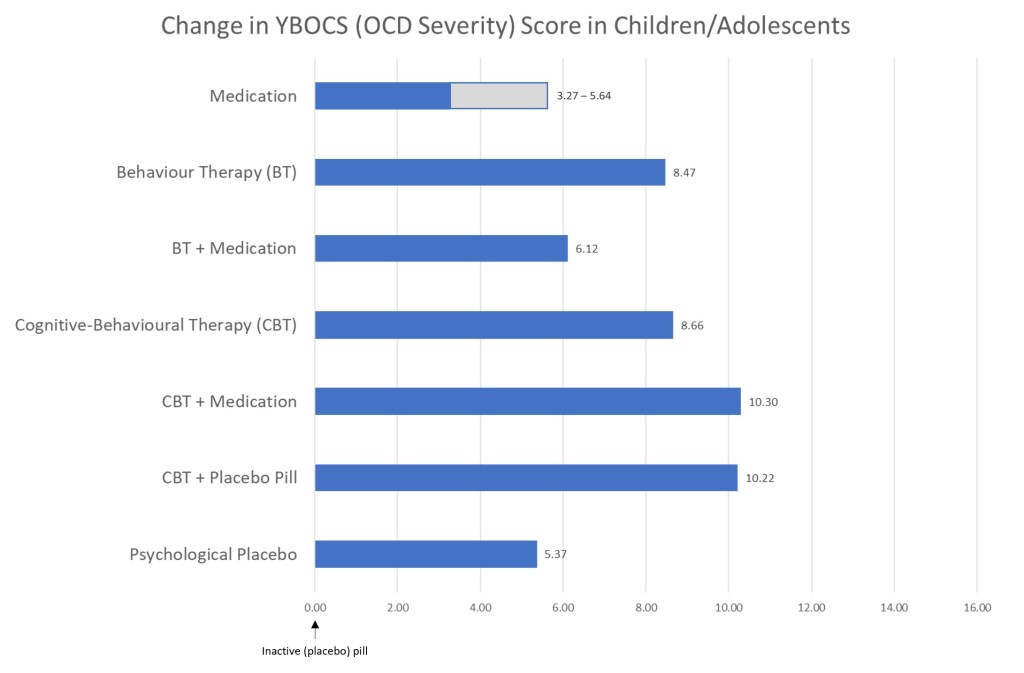
In treating OCD in children and adolescents, CBT in combination with medication (or a placebo pill) were the most efficacious, followed by CBT alone and behavioural therapy. Behaviour therapy in combination with medication did not perform quite as well, and was comparable to medication alone or psychological placebo.
Factors influencing treatment decision
From the findings, we can see which interventions should be prioritized when treating OCD in adults or children and adolescents. However, having said that, several factors obfuscate this seemingly straightforward decision – costs, time, attrition, and access.
While the costs identified in the UK study may not be generalizable across all countries, the authors found that the overall cost of medication is slightly cheaper than psychotherapy (BT, CT, CBT) when treating OCD. One reason could be the duration and number of sessions required in psychotherapy before any reasonable improvements could be observed. The study found that the number of sessions of psychotherapy required by participants ranged from around 10 to 40.
Given the number of sessions of psychotherapy required in the treatment of OCD, time and commitment becomes an issue. Some people may not have the ability to commit up to 40 hours to psychotherapy in the short term. This makes medication a more practical and sustainable alternative as treatment. While it is definitely possible to stretch the number of sessions over an extended period of time, doing so generally reduces the effectiveness of therapy. For example, someone who attends psychotherapy weekly or fortnightly might see recovery or remission come sooner than one who has monthly sessions.
Attrition, or dropping out of treatment midway, is also a possible challenge in treating OCD. Given the number of sessions required by psychotherapy, as well as the potential costs involved, a sizeable number of individuals may not complete the required number of sessions to fully recover from OCD or to enter remission. For others, the prospect of challenging their fears through Exposure and Response Prevention might be overwhelming, leading to attrition as well. Consequently, individuals may seek alternatives (e.g. medication) to the more efficacious BT.
Lastly, having frequent and timely access to psychotherapy may not be possible for many. Depending on where you live, it might be easier to find a primary healthcare practitioner who could dispense medication than it is to find a therapist. However, with the advent of internet-delivered psychotherapy taking hold, we may soon see increased accessibility to such services in more rural places.
While the above factors may suggest medication as the cheaper, less time intensive, and more accessible intervention, the potential side effects and tolerability of medication should also be considered to have a balanced perspective.
To sum up, the current study has shown that all the above listed interventions are effective in treating OCD – some more than others. While we should ideally choose interventions that have the best efficacy, practical constraints may influence why people may have to choose alternatives. Regardless, seeking help is the most important first step in treating OCD.
Eugene

One thought on “Research Review: Evidence-based treatment of Obsessive-Compulsive Disorder (OCD)”